 |
|
|
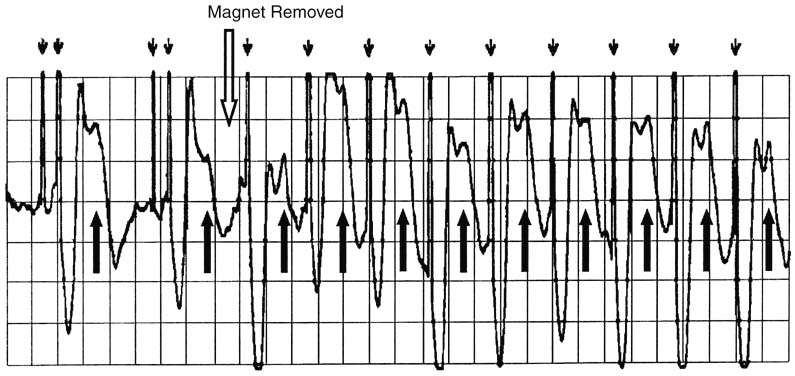
Figure 35-4
A pacemaker-mediated tachycardia (PMT) follows magnet
removal from a pacemaker. This patient had a dual chamber pacemaker implanted for
atrioventricular (AV) nodal disease, and she was pacemaker dependent for ventricular
activity. She had a sinus rate of 75 beats/min before the magnet application with
appropriate ventricular pacing (strip not shown). Her programmed AV delay is 200
msec. With magnet application, her pacemaker produced asynchronous AV sequential
pacing (DOO mode) at a rate of 60 beats/min. This strip is from an electrocardiographic
recorder that enhances the pacemaker artifact with small, downward
arrows. Because the asynchronous magnet rate of this device is lower
than her intrinsic atrial rate, many of the atrial pacing stimuli were applied during
an atrial refractory period (i.e., functional noncapture). A consequence of atrial
noncapture can be retrograde AV nodal conduction, with depolarization of the atria
after the depolarization of the ventricles. The retrograde P waves are shown with
the upward arrows. While the magnet is applied,
this retrograde depolarization of the atria is ignored. Shortly after the magnet
was removed (open arrow), there was a paced ventricular
event, followed by retrograde AV nodal conduction. With the ensuing depolarization
of the atria from this retrograde conduction, the pacemaker sensed an atrial event
and responded by pacing the ventricle 200 msec later. Another retrograde P wave
appears, and each pace in response to a retrograde P wave created yet another ventricular
pace. The result is a PMT at the upper tracking rate (programmed here to 130 beats/min)
of the pacemaker. PMT from retrograde AV nodal conduction can occur in any DDD or
VDD device with magnet removal, with a premature ventricular contraction, or with
a noncaptured atrial pace. Treatment of this PMT entails reapplication of the magnet.
Some pacemakers can be programmed to eventually break PMT by delaying one AV cycle
when pacing at the upper tracking limit.
|
|