 |
|
|
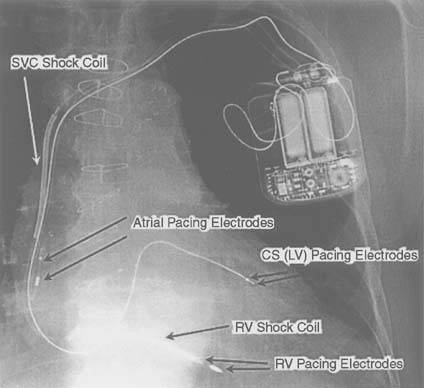
Figure 35-2
A defibrillator system with biventricular (BiV) pacemaker
capability. Three leads are placed: a conventional, bipolar lead to the right atrium;
a quadripolar lead to the right ventricle (RV); and a lead to the coronary sinus
(CS). This system is designed to provide "resynchronization therapy" in the setting
of a dilated cardiomyopathy with a prolonged QRS (and frequently with a prolonged
PR interval). The bipolar lead in the right atrium performs sensing and pacing functions.
Likewise, the bipolar tip in the RV performs pacing and sensing functions. The
lead in the CS depolarizes the left ventricle (LV). In most BiV devices, both ventricles
are depolarized simultaneously, because the electrode on the RV lead are connected
in parallel with the electrode on the CS lead. This parallel connection can cause
ventricular oversensing (and inappropriate antitachycardia therapy) in an implantable
cardioverter-defibrillator (ICD) if the pacemaker fails to depolarize one or both
of the ventricular chambers. The presence of "shock" conductors on the RV lead,
called coils, in the RV and the superior vena cava
(SVC) distinguish a defibrillation system from a conventional pacemaking system.
Typically, the SVC shock coil is electrically identical to the defibrillator case,
called the can. When the defibrillation circuitry
includes the ICD case, it is called an active can configuration.
|
|