 |
|
|
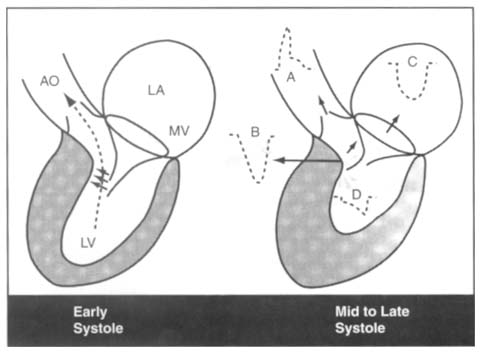
Figure 50-19
Left, Proposed mechanism
of mitral leaflet systolic anterior motion (SAM) in early systole in hypertrophic
cardiomyopathy. Ventricular septal hypertrophy causes a narrowed outflow tract,
as result of which ejection velocity is rapid and the path of ejection (dashed
line) is closer to the mitral leaflets (MV) than normal. This results
in Venturi forces (three short oblique arrows in
the outflow tract) drawing the anterior or posterior mitral leaflets, or both, toward
the septum. Subsequent mitral leaflet-septal contact results in obstruction to left
ventricular (LV) outflow and concomitant mitral regurgitation as seen in the right
panel. By midsystole, SAM-septal contact is well established and is causing marked
narrowing of the LV outflow tract with obstruction to outflow. LA, left atrium;
AO, aorta. Right, Proximal to the level of SAM-septal
contact, converging lines indicate acceleration of
the jet just proximal to the obstruction and narrowing of the jet width. Distal
to the obstruction, the arrow and diverging
lines indicate a high-velocity flow that emanates from the site of SAM-septal
contact and is directed posterolaterally at a considerable angle from the normal
path of aortic outflow. In late systole, although forward flow continues into the
outflow tract and aorta, the volume of flow is much less than in the early nonobstructed
systole. Typical Doppler flow patterns are shown. A, integrated Doppler flow signal
in the ascending aorta; B, high outflow tract velocity recorded by continuous-wave
(CW) Doppler at the site of SAM-septal contact; C, presence of mitral regurgitation
recorded by CW Doppler; D, late systolic velocity peak that can be recorded in the
apical region of the left ventricle. (Redrawn from Wigle ED: Hypertrophic
cardiomyopathy: A 1987 viewpoint. Circulation 75:312, 1987.)
|
|